

")

Focused.Accurate.Compliant.
Dermatology
Billing Services
Specialized medical billing solutions for dermatology practices.
Improve cash flow, reduce denials, and stay compliant so you can focus on your clients.
99% Claim Success Rate
Schedule an Appointment
Dermatology Medical Billing Services
Dermatology is one of the few specialties where a single patient visit can produce a shave biopsy, two lesion destructions, a punch biopsy of a separate site, and a cosmetic Botox conversation, all inside fifteen minutes. Each of those events bills differently. Some go to the payer, some go to the patient, and a few will get denied if the modifier or the lesion measurement is off by a hair. That density is exactly why generic billing companies bleed dermatology practices, and it’s why most of the revenue you’re missing isn’t lost at the front desk. It’s lost in the coding.
Mediflows handles dermatology billing the way it actually works in a real clinic: medical and cosmetic claims kept in separate lanes, every excision coded off pathology and excised diameter, Mohs billed stage by stage, and denials worked the same week they post instead of the following month. We charge a flat monthly fee, not a slice of your collections, so the more you earn, the less you pay us as a percentage of it.
Dermatology medical billing is the process of coding, submitting, and collecting payment for dermatology services across two revenue streams: medically necessary care (biopsies, excisions, lesion destruction, Mohs surgery, phototherapy) billed to insurance, and cosmetic procedures (Botox, fillers, elective laser) billed directly to patients. Because dermatology visits often stack multiple procedures with strict modifier and documentation rules, it carries a higher denial risk than most specialties.
What Is Dermatology Medical Billing?
Dermatology medical billing is the full revenue cycle for a skin practice, from the moment a patient is scheduled to the moment the last dollar is collected and the account closes. On paper that sounds like any specialty. In practice, dermatology is unusual because the same provider, in the same room, on the same day, routinely performs services that belong to completely different payment systems.
A medical visit for a suspicious mole is a covered service. The Botox the patient asks about while they’re in the chair is not. A biopsy is reimbursed by insurance; the cosmetic laser they book for next month comes out of their own pocket. A billing team that treats all of this as one undifferentiated pile of claims will misroute charges, trigger denials for cosmetic services sent to payers, and quietly leave self-pay revenue uncollected.
Good dermatology billing keeps those streams clean. It codes each encounter off the documentation and the pathology report rather than off habit, applies the right modifiers when an E/M service and a procedure happen together, tracks Mohs by surgical stage, and reconciles the technical and professional components when pathology is read in-house. Get those mechanics right and the practice collects what it earned. Get them wrong and the leakage compounds, one underpaid claim at a time.
Why Dermatology Billing Is More Complex Than Other Specialties
Most specialties have a predictable claim shape. A cardiology consult, an orthopedic post-op, a primary care wellness visit, these follow patterns a competent biller can learn quickly. Dermatology doesn’t behave that way, and the reasons are baked into how the medicine is practiced.
The first reason is volume per visit. Dermatologists see a lot of patients in a day and frequently perform several billable procedures on each one. That stacking creates modifier requirements, bundling edits, and multiple-procedure reductions that have to be handled on every claim. Miss one and the whole claim can reject.
The second reason is the procedure mix itself. A short list of what shows up on a normal day:
Biopsies. Tangential (shave), punch, and incisional biopsies each have their own base code, and additional lesions taken with the same technique need add-on codes. You can only bill one primary biopsy code per encounter, which trips up coders who try to bill a primary code for every lesion.
Lesion removals. Excision codes split into benign and malignant, then split again by anatomic site and by the excised diameter, which includes the surgical margins, not just the lesion. The measurement has to be taken before the specimen goes into formalin, because tissue shrinks, and that one detail decides which code (and which reimbursement) applies.
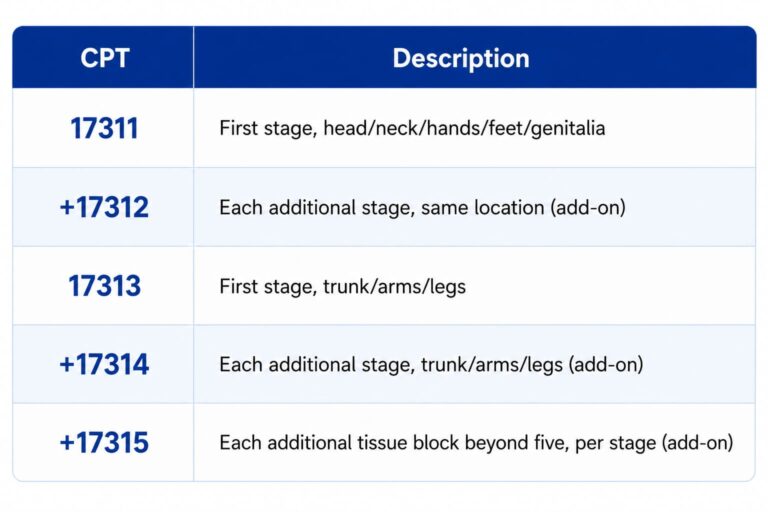
Mohs surgery. Mohs is billed stage by stage. The first stage on the head, neck, hands, feet, or genitalia uses one base code; the trunk and limbs use another; each additional stage and each extra block of tissue beyond five carries its own add-on. Incomplete stage documentation is one of the most common reasons Mohs revenue is left on the table.
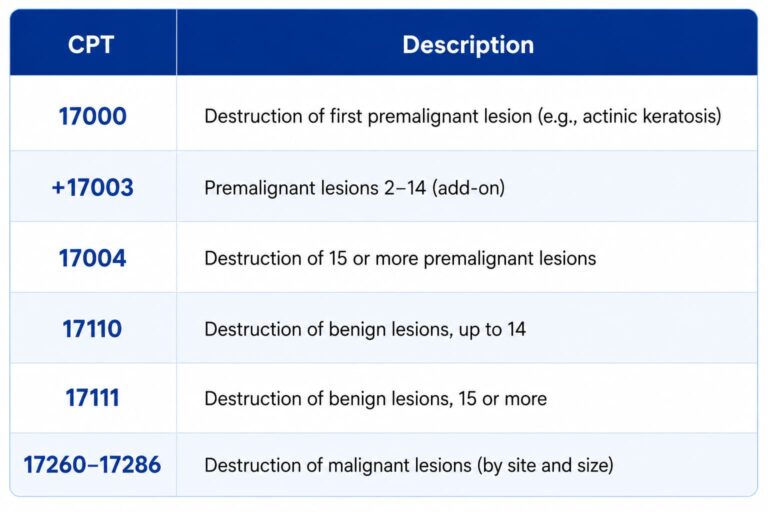
Cryotherapy and destruction. Destroying actinic keratoses, warts, and other lesions is coded by whether the lesion is premalignant, benign, or malignant, and by how many were treated. The benign and premalignant code families look almost identical, which is why experienced derm coders keep a quick-reference chart at their desk.
Cosmetic procedures. Botox, dermal fillers, elective laser, and chemical peels are typically self-pay and excluded from insurance. Billing them to a payer is a fast route to a denial and, if it becomes a pattern, a compliance problem.
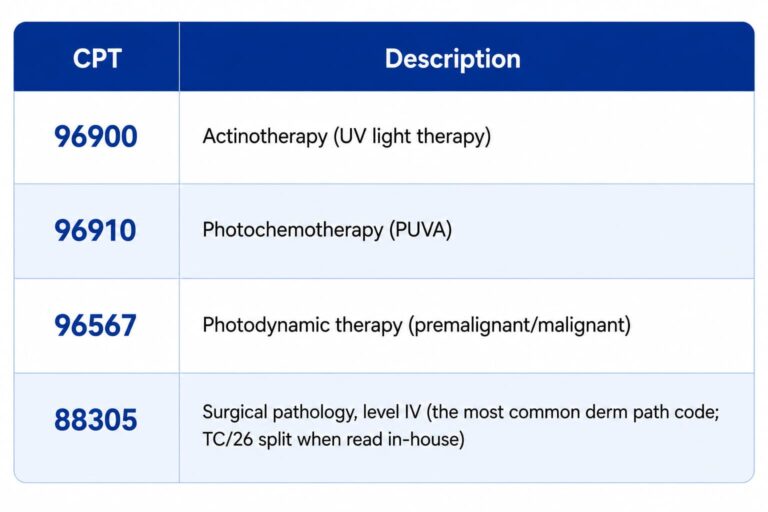
Phototherapy and PDT. UV light therapy, photochemotherapy, and photodynamic therapy each have specific codes, and PDT in particular has to be documented as medically necessary rather than cosmetic to be paid.
The third reason is documentation sensitivity. Payers scrutinize dermatology because so much of
it sits near the cosmetic line. Medical necessity, lesion counts, sizes, and margins all have to be
in the note, or the claim is exposed in an audit even when the care was perfectly appropriate.
Put those three together and you have a specialty where coding accuracy isn’t a nice-to-have. It’s the difference between a clean claim and a denied one, on nearly every patient, every day.
Talk to a Dermatology Billing Specialist about your current denial rate. Schedule a consultation or call 888-305-4084.
Common Dermatology Billing Challenges
Across dermatology practices, the same handful of problems account for most of the lost revenue. None of them are exotic. They’re the predictable result of a high-volume, highcomplexity specialty being billed by people who don’t live in it every day.
Claim denials from coding errors.
Modifier mistakes.
Documentation gaps.
Prior authorization failures.
Cosmetic versus medical confusion.
Slow AR follow-up.
| Challenge | Why it happens | Revenue impact |
|---|---|---|
| Coding errors | High procedure volume, complex code families | Denials and rework |
| Modifier 25 / 59 misuse | Stacked services on most claims | Bundled or denied lines |
| Documentation gaps | Missing counts, sizes, medical necessity | Audit exposure, takebacks |
| Prior auth misses | Biologics and select procedures | Full claim denial |
| Cosmetic vs medical | Two payment systems, one visit | Denied claims + uncollected self-pay |
| Aged AR | High claim count, slow follow-up | Lower net collection rate |
Dermatology CPT Codes Every Practice Should Know
These are the workhorse codes in a dermatology practice. They’re current for 2026, but they’re a reference, not a substitute for coding off the actual documentation and pathology in each case. Anatomic site and excised diameter change the specific excision code, so the ranges below resolve to a single code once those details are known.
Skin biopsies
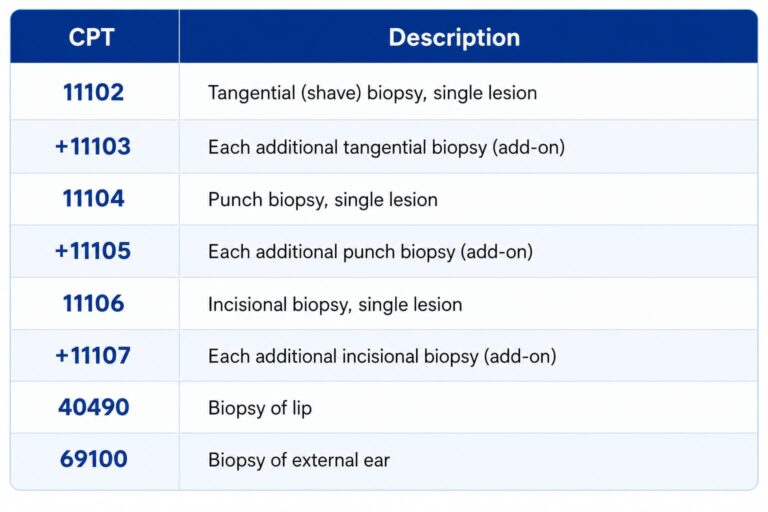
A common mistake: billing a primary biopsy code (11102, 11104, or 11106) for every lesion. Only the first lesion of a given technique gets the primary code. Additional lesions use the matching add-on.
Lesion destruction
Lesion excision
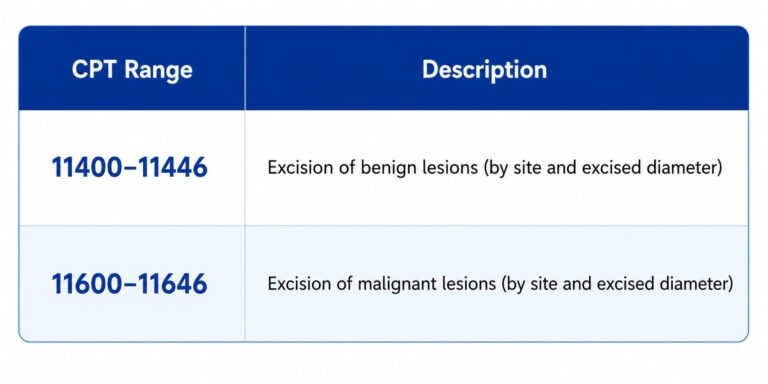
The code depends on three things: benign versus malignant (confirmed by pathology), the anatomic location, and the excised diameter, which is the lesion plus the surgical margins. Measure before excision.
Mohs micrographic surgery
Wound repair after excision

Phototherapy, PDT, and pathology
Evaluation and management
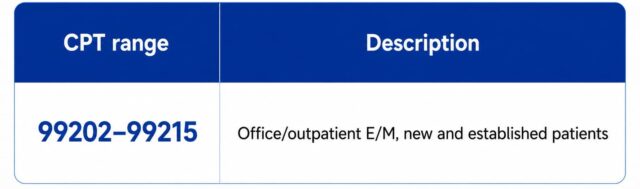
When an E/M service is significant and separately identifiable from a same-day procedure, it’s
reported with modifier 25. That single modifier is responsible for a large share of dermatology’s
modifier-related denials, in both directions.
ICD-10 Coding in Dermatology
CPT describes what you did. ICD-10 describes why. Every dermatology claim needs both, and they have to be clinically consistent, because a procedure code that doesn’t match the diagnosis is a denial waiting to happen. A few diagnoses that show up constantly:
L57.0
Actinic keratosis (pairs with destruction codes 17000–17004)
D22.x
Melanocytic nevi, by site (e.g., D22.5, trunk)
D23.x
Other benign neoplasm of skin
L82.x
Seborrheic keratosis
B07.x
Viral warts
C44.x
Other and unspecified malignant neoplasm of skin (basal cell, squamous cell)
L40.x
Psoriasis (relevant for biologics and phototherapy authorization)
A worked example: a shave biopsy of a melanocytic nevus on the trunk is 11102 (CPT) linked to D22.5 (ICD-10). The two have to agree. If pathology later returns malignant, the diagnosis and downstream codes change, which is why dermatology coding often can’t be finalized until the path report is back.
Medical vs Cosmetic Dermatology Billing
Dermatology medical billing is the full revenue cycle for a skin practice, from the moment a patient is scheduled to the moment the last dollar is collected and the account closes. On paper that sounds like any specialty. In practice, dermatology is unusual because the same provider, in the same room, on the same day, routinely performs services that belong to completely different payment systems.
A medical visit for a suspicious mole is a covered service. The Botox the patient asks about while they’re in the chair is not. A biopsy is reimbursed by insurance; the cosmetic laser they book for next month comes out of their own pocket. A billing team that treats all of this as one undifferentiated pile of claims will misroute charges, trigger denials for cosmetic services sent to payers, and quietly leave self-pay revenue uncollected.
Good dermatology billing keeps those streams clean. It codes each encounter off the documentation and the pathology report rather than off habit, applies the right modifiers when an E/M service and a procedure happen together, tracks Mohs by surgical stage, and reconciles the technical and professional components when pathology is read in-house. Get those mechanics right and the practice collects what it earned. Get them wrong and the leakage compounds, one underpaid claim at a time.
Talk to a Dermatology Billing Specialist about your current denial rate. Schedule a consultation or call 888-305-4084.
The Dermatology Revenue Cycle Management Process
Revenue cycle management is the end-to-end flow that turns a patient visit into collected, posted, and closed revenue. In dermatology, every step carries specialty-specific risk, so here’s how the cycle actually runs, stage by stage.
Scheduling
Eligibility verification
Prior authorization
Coding
Charge capture
Claims submission
Payment posting.
Denial management
AR follow-up
The dermatology revenue cycle in one line: schedule → verify eligibility → obtain prior auth
→ code from documentation → capture charges → submit clean claims → post payments →
manage denials → follow up on AR.
Why Dermatology Claims Get Denied
Denials in dermatology are rarely random. They cluster around the same root causes, which is good news, because patterns can be fixed. The table below covers the denials we see most often and what’s actually behind them.
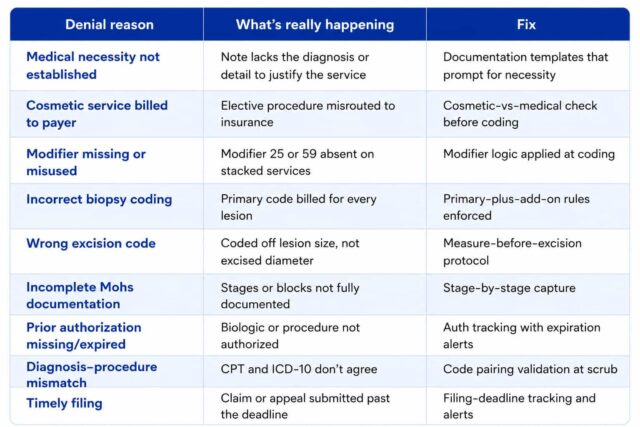
The throughline is that almost all of these are preventable at the coding and submission stage. Working denials matters, but preventing them is cheaper, and prevention is mostly a documentation-and-coding discipline problem, not a mystery.
How Mediflows Improves Dermatology Revenue
We don’t promise miracle percentages, and you should be skeptical of any billing company that
does without showing you the math on your own claims. What we do is run dermatology billing
with the specialty discipline it requires, and let the cleaner claims and recovered denials speak
for themselves.
Certified coders who know dermatology
Biopsy add-on rules, excision diameter coding, benign-versus-malignant logic, Mohs staging, modifiers 25 and 59, and the cosmetic line, coded by people who handle these every day rather than treating derm as just another specialty in the queue.
Denial recovery worked by root cause
Every denied dermatology claim is reviewed for why it denied (modifier, documentation, cosmetic misroute, authorization), corrected, and appealed with the clinical support to back it. Denial management is the part of our service we lead with, because it’s where most dermatology revenue is recoverable.
Faster, cleaner reimbursements
Claims are scrubbed against payer edits before they go out, so
the aim is first-pass acceptance rather than a cycle of submit, deny, appeal.
Lower AR days
Disciplined follow-up on outstanding claims keeps accounts from aging into
the hard-to-collect zone, which matters more in dermatology than almost anywhere because of
the sheer claim count.
Compliance you don’t have to think about
HIPAA-aligned handling of protected health
information, clean separation of cosmetic and medical billing, and documentation practices built to survive an audit.
Flat-fee pricing
Here’s the part that’s genuinely different. Most dermatology billing companies take a percentage of everything you collect, so when your practice has a great month, your
billing bill goes up too. We charge a flat monthly fee. Your cost is predictable, and as your collections grow, what you pay us shrinks as a share of your revenue. The incentive stays where it belongs.
Request a Free Billing Audit and see exactly where your dermatology revenue is leaking.
Start here or call 888-305-4084.
AI-Powered Dermatology Billing
Most of the “AI” in medical billing marketing is decoration. The places where it actually earns its keep in a dermatology workflow are narrow and specific, and worth being honest about.
Coding validation
Predictive denial prevention
Claim scrubbing
Revenue forecasting
Workflow automation
The honest framing: AI in dermatology billing is a way to catch errors earlier and work smarter, not a replacement for coders who understand the specialty. The practices that get value from it are the ones that already have clean processes for it to support.
Why Outsource Dermatology Medical Billing?
The case for outsourcing dermatology billing isn’t ideological. It’s arithmetic, and it comes down to whether an in-house team can match the specialty depth and consistency that dermatology demands without costing you more than it returns.
In-house billing means salaries, benefits, software, ongoing coding education, and coverage when someone is out sick or quits, all carried by the practice. It also means your billing knowledge lives in a small number of heads. When the person who understood Mohs staging leaves, that knowledge walks out with them. For a high-complexity specialty, that concentration of risk is real.
Outsourcing converts that fixed overhead into a service cost and spreads specialty expertise across a team that does dermatology coding all day. The trade-off you’re weighing is the cost of the service against the revenue recovered through cleaner claims, fewer denials, and faster collections, plus the staff time freed to run the practice instead of chasing payers.
Here’s the part that usually decides it: most billing companies charge a percentage of collections, which means the better your practice does, the more outsourcing costs you in absolute dollars. A flat-fee model removes that tax on your own growth. You pay a predictable monthly amount, and the upside from improved collections stays with the practice.
Quick checklist: is outsourcing right for your practice?
If you checked three or more, an outside dermatology billing partner is worth a conversation
Why Choose Mediflows Billing Solutions
There are a lot of dermatology billing companies. Here’s the short version of what makes the decision with us different.
We lead with denial management because that’s where the recoverable money is, and we work denials by root cause the same week they post, not in a monthly batch. We keep cosmetic and medical billing in clean, separate lanes, which is the single most important thing a dermatology biller can get right. Our coders are certified and work dermatology specifically, so biopsy addons, excision diameters, and Mohs staging are routine rather than research projects.
And we charge a flat monthly fee instead of a percentage of your collections. That one structural choice means our interests don’t quietly diverge from yours as you grow, and your billing cost stays predictable month to month. You also get a clear view of your own numbers, claims, denials, and AR, rather than a PDF summary once a month.
If you want to see what that looks like against your actual claims, the audit is free and the first finding usually pays for the conversation.
Schedule Your Consultation with a dermatology billing specialist. Book a time or call 888-305-
4084.
Frequently Asked Questions
What is dermatology medical billing?
Dermatology medical billing is the process of coding, submitting, and collecting payment for dermatology services. It covers two streams: medically necessary care like biopsies, excisions, and Mohs surgery billed to insurance, and cosmetic procedures like Botox and fillers billed directly to patients. The dual stream structure and stacked procedures make it more denial-prone than most specialties.
How much does dermatology medical billing cost?
Pricing varies by model. Many billing companies charge a percentage of collections, commonly in the range of 4% to 10%. Mediflows uses flat monthly pricing instead, so your cost stays predictable and doesn't rise just because your collections grew. Request a quote for pricing matched to your practice size and claim volume.
What CPT codes are used in dermatology?
Core dermatology CPT codes include 11102-11107 for biopsies, 17000-17004 and 17110-17111 for lesion destruction, 11400-11446 and 11600-11646 for benign and malignant excisions, and 17311-17315 for Mohs surgery. Office visits use 99202-99215, often with modifier 25 when an E/M is separately identifiable from a same-day procedure.
What is Mohs surgery billing?
Mohs billing reports the procedure stage by stage. The first stage on the head, neck, hands, feet, or genitalia is 17311; on the trunk or limbs it's 17313. Each additional stage uses an add-on code (17312 or 17314), and 17315 covers extra tissue blocks beyond five. Complete documentation of each stage is required to be paid fully.
What causes dermatology claim denials?
The most common causes are missing medical necessity documentation, cosmetic services billed to insurance, modifier 25 or 59 errors, incorrect biopsy or excision coding, incomplete Mohs documentation, missing prior authorization, and diagnosis-procedure mismatches. Most are preventable at the coding and submission stage rather than at appeal.
Is outsourcing dermatology billing worth it?
For most practices, yes, especially if the clean claim rate is below 95%, denials are climbing, or AR days are rising. Outsourcing converts fixed billing overhead into a service cost and spreads specialty expertise across a dedicated team. A flat-fee partner is particularly worth it for growing practices, because percentage pricing taxes your own growth.
What's the difference between medical and cosmetic dermatology billing?
Medical dermatology (biopsies, excisions, medically necessary procedures) is billed to insurance. Cosmetic dermatology (Botox, fillers, elective laser) is self-pay and excluded from coverage. They follow different rules, and a billing workflow has to separate them at the point of service to avoid both payer denials and uncollected patient balances.
What is a good clean claim rate for a dermatology practice?
A healthy clean claim rate is 95% or higher, with high-performing practices reaching 97% to 99%. A rate in the 80s usually signals coding or documentation problems concentrated in a few denial reasons, which is fixable once those reasons are identified.
What are modifiers 25 and 59 in dermatology billing?
Modifier 25 indicates a significant, separately identifiable evaluation and management service performed on the same day as a procedure. Modifier 59 indicates a distinct procedural service that isn't normally reported together with another. Both are common in dermatology because visits often stack an exam with one or more procedures, and misusing either causes denials
Do dermatology billers handle cosmetic procedures?
Yes. A dermatology billing partner manages cosmetic services as self-pay, including patient statements, point-of-service collection, and invoicing for non-covered procedures, while keeping them cleanly separated from insurance claims. This prevents cosmetic services from being denied by payers and prevents self-pay balances from aging into bad debt.
How long does it take to switch dermatology billing companies?
Transition typically takes a few weeks, depending on practice size, EHR or practice management system, and payer enrollments. A good onboarding process maps your current workflow first and runs in parallel so claims keep going out during the switch, minimizing disruption to cash flow.
Does dermatology billing require prior authorization?
Some of it does. Biologics for conditions like psoriasis, certain phototherapy regimens, and select surgical procedures often require prior authorization. Missing or expired authorizations are a frequent denial cause, so tracking authorization status and expiration dates is part of a sound dermatology billing workflow.
What is the excised diameter in dermatology excision coding?
The excised diameter is the size of the lesion plus the surgical margins, not just the lesion itself. It's one of the three factors (along with benign vs malignant and anatomic site) that determine the excision code. It must be measured before the specimen is removed, because tissue shrinks once it's placed in formalin.
How do you bill multiple biopsies in one visit?
Bill one primary biopsy code per technique, then use add-on codes for additional lesions taken with the same technique. For example, two shave biopsies are 11102 plus 11103. A shave and a punch in the same visit use 11102 and 11104. You cannot bill a primary code for every lesion.
Is dermatology billing HIPAA compliant with Mediflows?
Mediflows follows HIPAAaligned practices for handling protected health information, including secure systems and clean separation of medical and cosmetic billing data. Specific compliance documentation, including business associate agreements, is provided as part of onboarding. (See pre-publish note regarding legal document review.)
What KPIs should a dermatology practice track?
Track first-pass acceptance rate, clean claim rate, net collection rate, days in AR, and denial rate. Healthy targets are 95%+ acceptance and net collection, AR days under 40, and a single-digit denial rate. These five metrics reveal where revenue is leaking and whether your billing is actually improving.
Can small or solo dermatology practices use outsourced billing?
Yes. Solo dermatologists, multi-provider clinics, and multi-location groups all use outsourced billing. Flat-fee pricing in particular suits smaller practices that want predictable costs and don't have the volume to justify a full in-house billing team with deep dermatology coding expertise.
How does AI help with dermatology billing?
AI helps narrowly but usefully: validating codes before submission, flagging claims likely to deny based on payer and code patterns, scrubbing claims against payer edits, and forecasting revenue from clean historical data. It supports coders rather than replacing them, and it works best in practices that already have disciplined billing processes.
You Focus on Patients. We’ll Manage Billing
At Medi Flows, we are dedicated to delivering exceptional billing support for over 20 years, we have been a offering comprehensive medical services in USA
About Us
Mediflows has been offering comprehensive billing and revenue cycle solutions across a wide range of specialties all over USA.
Contact Info
Serving All Across The United States