

")

- mediflows
- billing cost
- May 22, 2026
- No Comments
Blog Details
Medical Billing Services for Small Practices: What Actually Matters in 2026
A solo provider clearing $480,000 in net collections at a 6% billing rate pays roughly $28,800 a
year for billing. The same provider running a 92% net collection rate instead of 84% pulls in an
extra $38,400. That recovered revenue is bigger than the billing fee itself.
That math is the only thing that matters. Not “are you outsourcing.” Not “what’s your percentage.” But: is your billing actually working?
This guide is for the practice owner or office manager who’s tired of vague vendor pages,
percentage-of-collections lock-in, and monthly PDFs that arrive on the 5th and tell you nothing
useful. What follows is what a small-practice billing engagement should look like in 2026, what
to pay, which KPIs to demand, the red flags hiding in standard vendor contracts, and how to
switch billers without your AR cratering for 90 days.
What "Small Practice" Means for Billing
There’s no clean industry definition. For revenue cycle purposes, a small practice usually fits
these markers:
One to five providers.
300 to 1,500 claims per month.
One to three admin staff (or zero, if fully outsourced).
$250K to $3M in annual net collections.
The reason size matters: billing problems compound faster at this scale. A 500-bed hospital can absorb a 5% denial rate. A two-provider family medicine clinic cannot. When margins are tight and your one biller goes on leave, the revenue engine stalls. Most enterprise RCM companies built their pricing and workflows for groups 5–10x your size and will quietly deprioritize your account once you sign.
According to the AMA’s 2024 Physician Practice Benchmark Survey, only 42.2% of US physicians worked in private practices in 2024, down from 60.1% in 2012. Most of that shift was small practices losing the back-office fight. Billing is one of the main reasons.
The Real Cost of Bad Billing at a Small Practice
Pull your last 90 days of payer remits and check three numbers.
Clean claim rate is the percentage of claims paid on first submission with no rework. The industry-acceptable floor is 95%. MGMA’s high-performer benchmark is 98%+. At 85%, you’re spending roughly 13% of your AR cycle on rework that shouldn’t exist.
Days in AR measures average time from claim submission to payment. Best in class runs under
30 days. Past 45 days, you’re bleeding. Past 60, you have a structural problem.
Net collection rate compares what you actually collected against what you contractually should have. A healthy small practice runs 95–97%. Below 92% means you’re writing off money you earned.
Take a $1.2M practice running an 87% net collection rate. That’s $96,000 a year walking out the door, equivalent to a part-time clinician’s revenue. It doesn’t show up on the P&L as “lost.” It shows up as “what we collected,” with no benchmark to compare against. That’s exactly how it stays invisible.
In-House vs. Outsourced Medical Billing: When Each Makes Sense
This isn’t a religious debate. The honest answer depends on volume, specialty, staff stability, and what you actually want to spend your week on.
When in-house billing works
Keep billing in-house if:
- You have a tenured biller (5+ years) experienced in your specialty
- Your specialty has predictable coding and a limited payer mix
- Your claim volume justifies a full-time billing role (roughly 1,500+ claims/month per biller)
- You have a real backup plan when that biller takes vacation, gets sick, or quits
The catch: a competent in-house biller in the US costs $52,000–$65,000 fully loaded with benefits. Practice management software runs $200–$1,500 per provider per month. Add clearinghouse fees, ongoing training, and the productivity hit when they leave. The “free inhouse biller” idea is fictional.
When outsourcing makes more sense
Outsourcing usually wins for:
· Solo or 2–3 provider practices
· Specialties with heavy modifier or payer-policy work (orthopedics, cardiology, behavioral health, ASC, pain management)
· Practices that have cycled through three billers in two years
· Denial rates above 7%
· Operations where AR aging isn’t visible in real time
The argument against outsourcing is loss of control. The argument for it is that you didn’t go to medical school to learn appeals language for CO-97 bundling denials
The hybrid model
A few practices run this well: in-house staff handles front-end work (eligibility, charge entry, patient questions), and an outsourced team handles coding review, claims submission, denial work, and AR follow-up. Your front office stays your front office. The back-office expertise becomes someone else’s problem to staff and retain.
How Medical Billing Services for Small Practices Actually Work
Here’s what a competent billing partner does, end to end, for one patient encounter.
- Eligibility verification (ANSI 270/271). Ideally 48 hours before the visit. Confirms active coverage, copay, deductible status, and prior auth requirements. Catches the “patient changed jobs in January, plan switched” problem before the visit happens.
- Prior authorization. Required for imaging, surgery, specialty drugs, behavioral health sessions past a threshold, and most expensive procedures. Document the auth number, effective dates, units approved, and CPT codes covered. Skipping this is a top-three denial source.
- Charge capture and coding. Translating the provider’s documentation into clean CPT, HCPCS, ICD-10, and modifier combinations. Most denials get manufactured here. Common landmines: modifier 25 (significant separate E/M on the same day as a procedure), modifier 59 (distinct procedural service), POS 02 vs. 10 for telehealth, and time-based coding documentation gaps.
- Clearinghouse scrubbing and submission (ANSI 837). Claims hit edits before reaching the payer. A solid biller’s clearinghouse clean-claim rate should run 98%+.
- Payment posting (ANSI 835/ERA). Automated posting of payments, contractual adjustments, and denials to patient accounts. Manual posting is where small errors compound into reconciliation nightmares.
- Denial work. Categorize by CARC/RARC codes, identify root cause, then appeal or correct. The denial categories that matter most: CO-16 (missing information), CO-97 (bundled), CO-45 (over fee schedule), CO-50 (not medically necessary), and CO-29 (timely filing).
- AR follow-up. Work claims at 30, 45, and 60 days. Past 90 days, recovery rate drops sharply. Past 120, you’re usually writing them off.
- Patient statements and collections. Clean statements, payment plan options, soft collections at 30/60/90 day intervals.
The full loop should run 18-25 days from date of service to payment. If yours is running 45+, something is broken in one of those eight steps.
In-House vs. Outsourced Medical Billing: When Each Makes Sense
Four common structures. Each has a use case and a way it can quietly cost you more than it should.
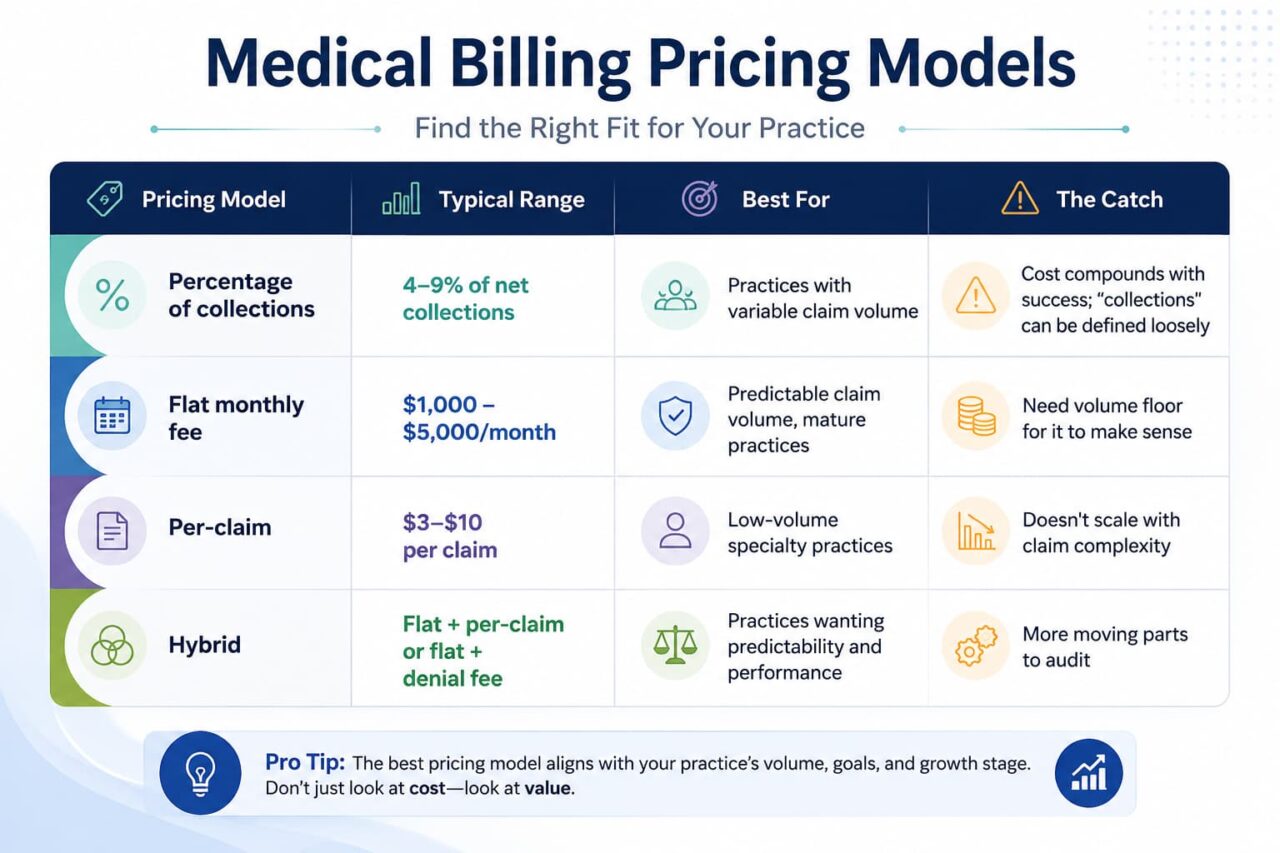
The percentage-versus-flat debate is more nuanced than most vendors will admit. Percentage aligns incentives: if they don’t collect, they don’t earn. That sounds clean until you do the math. A 6% rate on $1.2M is $72,000 a year, which is more than most small practices would pay an inhouse biller. As collections scale, percentage compounds against the practice.
Flat fee removes the compounding. The inverse risk is that if your vendor isn’t paid more when you collect more, what’s their incentive to chase that aging 90-day claim? The answer is contractual SLAs. Demand clean-claim rate, denial recovery percentage, and AR aging commitments in writing. Without those, flat fee turns into “set it and forget it” — which is also how revenue quietly leaks.
(Disclosure for the rest of this piece: Mediflows uses a flat-fee model. We’re biased here. The bias is informed by watching too many small practices pay 8% on $2M for a service whose dashboard refreshes once a month.)
Doing the pricing math properly
Don’t compare 5% versus 8% versus flat-fee in a vacuum. Compare effective cost per dollar collected.
- Vendor A: 5% rate, 84% net collection rate. On $1M billable, you collect $840K and pay $42K. Net to practice: $798K.
- Vendor B: 7% rate, 95% net collection rate. On the same $1M, you collect $950K and pay $66.5K. Net to practice: $883.5K.
The “more expensive” vendor leaves you $85,500 richer. The cheapest rate is almost never the cheapest deal. Run this calculation against any quote you receive.
KPI Benchmarks Every Small Practice Should Track
Your billing partner should publish these monthly at minimum, ideally daily via a live dashboard. If they can’t, that’s the answer to whether to keep them.
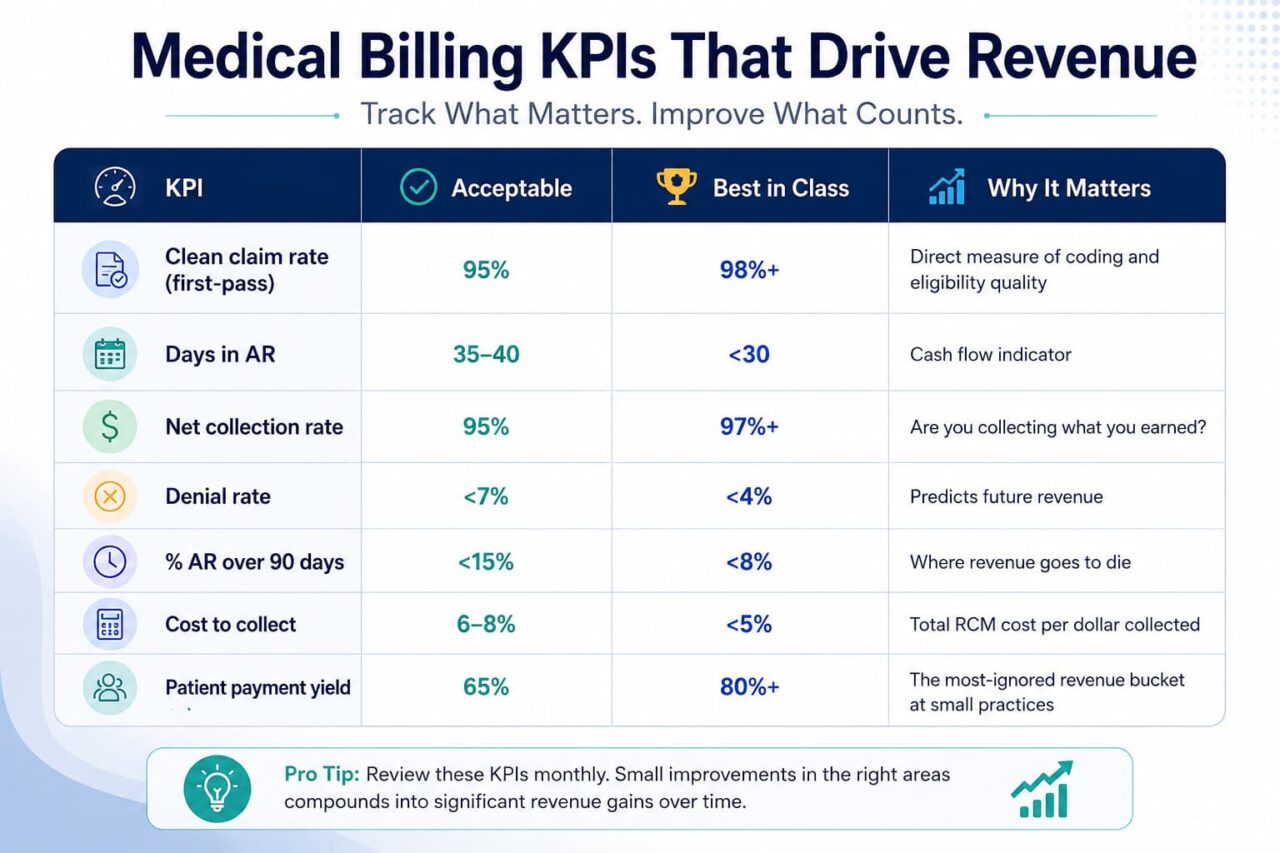
A vendor that can’t tell you these numbers for your account, this week, isn’t running an RCM operation. They’re running a claims-submission shop.
9 Questions to Ask Before Signing a Billing Contract
Most vendor pitches focus on the wrong things (years in business, number of clients, generic
“expertise”). Ask these instead.
- What’s your average clean-claim rate across your current client book not your best client?
- What’s your average net collection rate for practices in my specialty?
- Show me a sample dashboard. How often is it refreshed?
- Who specifically works my account? Is it a named team or a shared pool?
- How is the percentage defined in the contract — gross billed, net collections, or something else?
- What’s the minimum monthly fee, and when does it apply?
- How long is the term? What’s the termination notice period?
- What payer enrollments do I keep if we part ways?
- Can you give me three references at practices my size, in my specialty?
Question three matters most. A vendor that posts every claim, denial, and aging bucket daily is
structurally different from one that emails a PDF on the 5th of the month. The first runs an
operation. The second hopes you don’t look too closely.
Red Flags in Medical Billing Contracts
Read the contract. Or have an attorney read it. Watch for these patterns.
- Percentage of collections” defined as gross billed — you’d be paying on revenue you’ll never actually collect.
- Minimum monthly fees — a $2,500 minimum at a quoted 6% rate means you’re effectively paying 12%+ if your claim volume drops.
- Long auto-renewal clauses — a 60-day notice on a 36-month auto-renew is a trap dressed up as standard language.
- Vague exit terms — who owns the payer enrollments? Who has access to the historical claim data? If the contract doesn’t answer this, the vendor does.
- Credentialing billed separately as “additional” — some vendors quote billing fees, then add $300–$500/month per provider for credentialing.
- Proprietary software lock-in — if their system isn’t your system, your data is harder to extract on the way out.
- No SLAs on KPIs — if clean claim rate, denial recovery, and AR aging aren’t in the contract, they’re marketing copy.
How to Transition Without Losing Revenue: The 60-Day Playbook
Switching billers is the single highest-risk RCM project a small practice runs. AR can age 30–45 days during a botched transition. Done badly, you lose a full month of cash flow. Done right, you barely notice.
Switching billers is the single highest-risk RCM project a small practice runs. AR can age 30–45 days during a botched transition. Done badly, you lose a full month of cash flow. Done right, you barely notice.
Weeks 1–2: Parallel preparation
- Sign BAA with new vendor
- Coordinate payer EFT/ERA redirects (some payers take 4–6 weeks)
- Document current AR by aging bucket and payer
- Confirm PM/EHR access for new team
- Lock the cutover date with both vendors in writing
Weeks 3–4: Soft cutover
- New vendor begins working all new claims from the cutover date forward
- Old vendor continues working pre-cutover AR
- Daily sync between teams on payer-specific issues
- Eligibility verification handoff happens immediately
Weeks 5–6: AR transition
- Old vendor delivers a full AR aging report with claim-level notes
- New vendor begins working pre-cutover AR over 30 days old
- Cross-check posting reports daily
Weeks 7–8: Full handover
- All AR work moves to new vendor
- Old vendor exits with a final reconciliation
- Begin tracking new vendor’s KPIs against contracted SLAs
The biggest assumption to discard: your old vendor will not work hard during their last 30 days. Plan accordingly. Assume the AR you hand them stays where it is, and that you’ll be cleaning up tail claims for 90 days after exit.
Specialty Considerations for Small Practices
Different specialties carry different billing landmines. A few quick reads:
Family practice and internal medicine. High E/M volume, modifier 25 issues, chronic care management (CCM) and remote patient monitoring (RPM) chronically underutilized. Many small primary care practices leave $20K–$50K a year in CCM revenue uncoded.
Mental health. Time-based coding (90832 / 90834 / 90837), supervisory billing complexity, telehealth POS confusion. State Medicaid behavioral health rules are particularly inconsistent.
Pain management. Bundling rules around injections, NCCI edits, modifier 59 application, and payer prior auth that comes in aggressive.
Physical therapy. 8-minute rule documentation, modifier KX threshold management, plan-of-care compliance.
Ambulatory surgery centers. Facility vs. professional split, modifiers 50/RT/LT, payerspecific implant carve-outs.
Cardiology. High-RVU procedures with complex modifier requirements (26, TC, 59), cath lab prior auth, and supervision-level documentation.
If your billing partner can’t speak fluently about your specialty’s specific landmines on the discovery call, they’ll be learning on your account. That’s an expensive education.
Compliance, HIPAA, and Your BAA
The Business Associate Agreement is the legal document that makes your billing vendor
accountable for protecting PHI. Three things to verify before signing.
Breach notification timeline. The federal HIPAA minimum is 60 days. A serious vendor commits in writing to under 5 business days.
Subcontractor provisions. If any portion of the work is offshored or sub-contracted, the BAA has to disclose and cover it. A “we don’t offshore” claim without contract language is just a verbal promise.
Audit rights. You should have the right to request SOC 2 reports, access logs, and security documentation on demand.
Beyond HIPAA, state-level laws add obligations. California’s CMIA, Texas HB 300, and New York’s SHIELD Act all carry their own breach and security requirements. A billing partner that’s only “HIPAA compliant” without state-level awareness can expose you to liability you didn’t agree to carry.
What ROI Looks Like at Day 30, 60, and 90
Realistic timeline for a well-run engagement at a small practice.
Day 30. Clean claim rate stabilizing at 95%+. Denial categorization complete. Top 5 root causes
named with dollar values attached. Eligibility process tightened.
Day 60. AR aging shifting left (claims moving out of 60+ buckets). First batch of appeals returning paid. Patient statement process cleaned up.
Day 90. Net collection rate measurable and trending up. Days in AR moving toward 30. Monthly revenue 6–12% higher than baseline. KPI dashboard shows weekly improvement.
If you’re not seeing measurable movement on at least three KPIs by day 90, something is off. Either the historical data was dirtier than anyone admitted (often true) or the vendor isn’t doing the work they promised. Both are fixable, but only if you have the dashboard visibility to spot it.
What to Look For in a Medi Flows–Style Engagement
Quick positioning note. Mediflows runs a flat-fee model with a 30-day denial audit at the front of
every engagement and a live dashboard that refreshes daily. Not every practice needs that exact
structure. But every practice should demand what the structure represents: transparent pricing,
real visibility, accountability tied to KPIs, and no incentive on the vendor’s side to inflate claim
volume for higher fees.
If your current setup looks more like a monthly PDF with a vague summary and a chat thread
that goes quiet for two weeks, you’re a strong candidate for at least an audit. A 30-day look-back
at denial categories, payer mix, and AR aging usually tells you within a week whether your
current vendor is undercollecting.
Get a free 7-day revenue audit. Mediflows will show you, claim by claim, where your current billing is losing money. You keep the report whether or not you switch. Call 888-305-4084 or request your audit.
FAQ
Should a small practice outsource its medical billing?
Most small practices pay 4– 9% of net collections on a percentage model, $1,000–$5,000/month on a flat-fee model, or $3– $10 per claim on a per-claim model. The right model depends on claim volume, specialty complexity, and how predictable your revenue is. Compare effective cost per dollar collected — not just the headline percentage.
Should a small practice handle denial management in-house or outsource it?
Usually yes if you're solo or 2–3 providers, your specialty has heavy modifier or payer-policy work, your denial rate is above 7%, or you've cycled through billers recently. In-house can still win if you have a tenured specialty biller, predictable volume above 1,500 claims/month, and a real backup plan.
What is a good clean claim rate in 2026?
The industry-acceptable floor is 95%. MGMA's highperformer benchmark is 98%+. Below 90% means you have a systemic coding or eligibility problem, not a billing problem.
Categories
Tag Cloud