

")

- mediflows
- May 21, 2026
- No Comments
Blog Details
A step-by-step denial management playbook for small medical practices. No
enterprise team needed, just a clear process to recover what you are owed.
Denial Management for Small Practices: A Practical Playbook
Now multiply that stack by fifty Mondays. In a small medical practice, this is what denial management actually looks like. There is no dashboard and no denial department. There is a stack of EOBs and someone who needs to work it before patients start arriving at 8:30.
The big medical billing companies will hand you a brochure about their AI-powered denial intelligence platform and their team of seventy-five denial analysts. That advice is built for a four-hospital system. You have a coffee maker that needs descaling and a payer rep who never returns voicemails. This piece is the version of denial management that fits a small practice. No new software. No new hires. Just a clear process for recovering the money you are already owed.
The corporate blindspot
A two-provider practice has none of that. It has a front desk that also answers the phone. It has an office manager who also handles payroll, runs reports, and probably keeps the schedule. The enterprise advice does not translate, and the giants rarely notice.
This is where a smaller billing partner earns its keep. Not by selling you a dashboard with seventeen filters. By being a person who knows your top five payers, calls your office on Wednesdays, and reworks denials before they age out.
What actually happens to a denied claim in a small practice
This is the part the enterprise content skips. The problem is not that your team cannot fight denials. The problem is that nobody has a system for which denials to fight, in what order, and by when. So everything competes with everything else, and the easy wins drown.
A workable system has to fit on one page. The seven steps below are that page.
The seven-step denial management playbook

Step 1: Sort denials by dollar value, not date
The default in most practices is first-in-first-out. That feels fair. It also means you spend forty minutes on a $38 claim while a $620 claim ages another week.
Pull every open denial. Sort by amount. Work the top of the list first. Everything under your
write-off threshold (more on that in step 6) goes to a separate pile and gets batched once a
month.
Step 2: Identify your top three denial reasons
Most practices have a long tail of denial codes and assume the problem is everywhere. It usually is not. Run a report for the last 90 days and group denials by reason code. In nearly every small practice we have audited, three reasons account for more than 60% of denied dollars.
The top three are usually some combination of eligibility errors, missing prior auth, modifier mistakes, and registration problems. Once you know yours, you stop fighting denials one at atime and start fixing the upstream cause.
Step 3: Build a 48-hour rework rule
For every denial in your top three reasons, the clock starts when the EOB hits your inbox. The claim gets reworked or appealed within 48 hours. No exceptions.
This single rule does more for collections than any software. Denials that sit lose value fast.
Payer reps forget context. Timely-filing windows close. Patients move and stop answering the phone. The 48-hour rule keeps the freshest, most recoverable denials moving.
Step 4: Track appeals by payer
If you are sending three appeals a month to one payer and getting zero overturned, something is wrong with your appeal letter, your documentation, or the payer’s process. Keep a simple spreadsheet: date sent, payer, denial reason, dollar amount, outcome.
After 90 days you will see the pattern. Some payers overturn 80% of well-documented appeals. Some overturn 5% no matter what you send. Adjust where you spend your appeal time accordingly.
Step 5: Fix the front desk failure points
Eligibility and registration denials are not really billing problems. They are front desk problems. Run a 30-second eligibility check on every patient at check-in (most clearinghouses do this for free or close to it). Confirm insurance ID, group number, and coverage dates. Confirm the policyholder is who the patient says it is. Five questions, every visit.
If you find that one specific shift or one specific staff member has a denial rate twice the practice average, the conversation is training, not blame.
Step 6: Set a write-off threshold and stick to it
If a claim is denied for $14 and rework costs your office manager 25 minutes of focused work, you are losing money by chasing it. Pick a number. For most small practices, the threshold sits somewhere between $15 and $35. Anything below that gets written off in a monthly batch. Above it gets worked.
This is the rule most practices avoid because it feels like giving up. It is not giving up. It is
choosing which fights are worth fighting. The $14 claim is a distraction from the $620 claim.
Step 7: Review monthly, not quarterly
A 15-minute monthly review covers three numbers: total denied dollars, top three denial reasons, and average rework turnaround time. That is enough to spot a problem before it becomes a quarter-end disaster.
Quarterly reviews are too slow. By the time a September spike in eligibility denials shows up in the October report, you have lost ninety days of preventable claims.
In-house, enterprise giant, or nimble partner
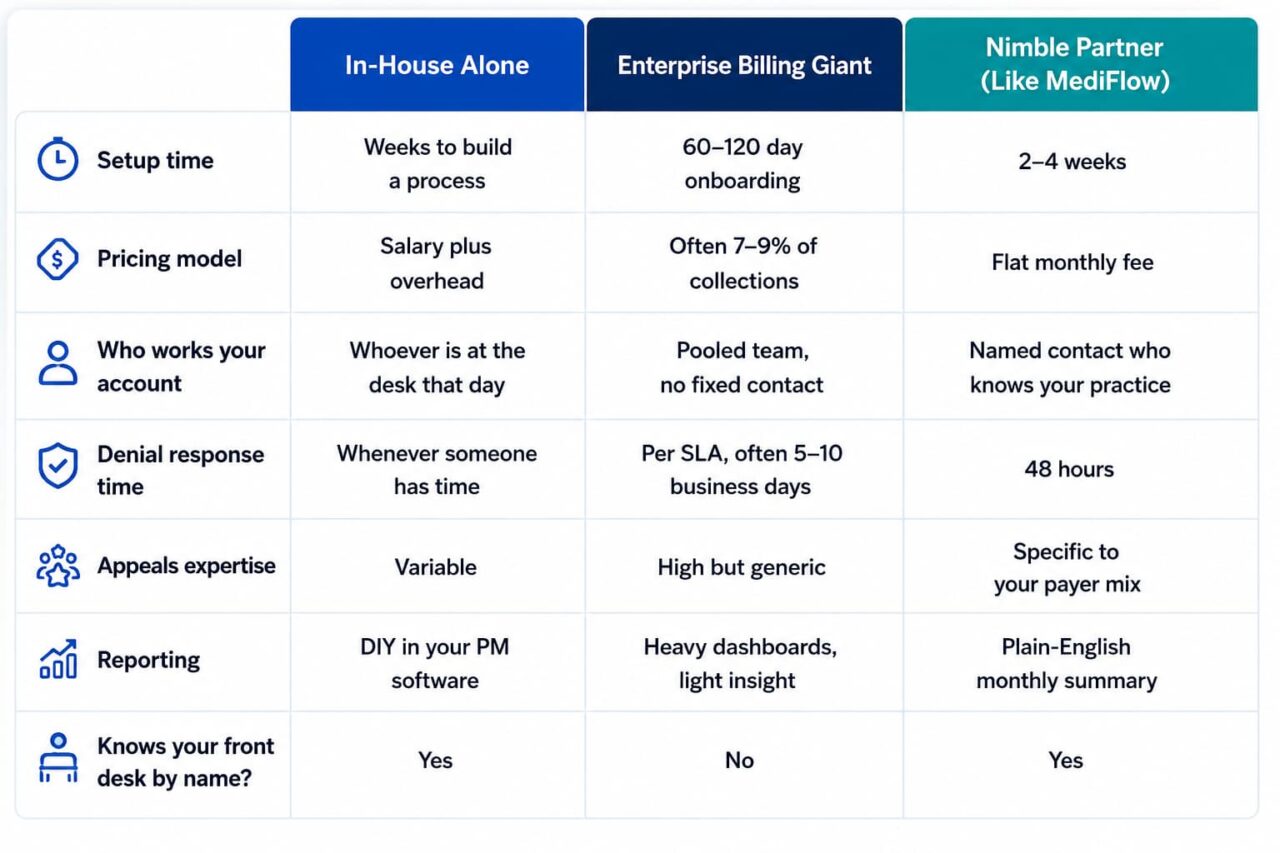
The in-house column works if you have the bench depth. Most small practices do not. The enterprise column looks attractive on the website and feels different by month three, when nobody returns the call about the modifier denial because your account got reassigned again. The middle option is a partner small enough to actually know your practice. For practices weighing the third column, our outsourced medical billing for small practices page walks through the dayto-day workflow.
When does outside help actually make sense
Bringing in a billing partner is not always the right answer. It makes sense when:
- Your aged AR over 90 days is more than 20% of total AR
- Your denial rate is above 8%
- Your office manager is working evenings and still falling behind
- You have lost a billing staff member and cannot fill the role
- You are adding a provider and the current workflow will not stretch
It is the wrong answer when the real problem is upstream. A billing company cannot fix a credentialing gap from downstream.
If your providers are not properly enrolled with the right payers, denials will keep coming. That is a provider credentialing and enrollment issue first, and a billing issue second.
For practices that need the whole revenue cycle handled eligibility, coding, claims, posting, AR, and denials a full revenue cycle management engagement covers all of it.
FAQ
What is a healthy denial rate for a small medical practice?
The industry benchmark is below 5%. Most small practices we audit start somewhere between 8% and 14%. Getting to 5% within six months is realistic with a consistent process and the playbook above.
Should a small practice handle denial management in-house or outsource it?
It depends on volume and bench depth. If your practice processes fewer than 100 claims a week and you have a stable office manager with the time, in-house can work. If volume is higher or your billing role has turned over more than once in two years, outsourcing usually costs less than the lost revenue from inconsistent denial work.
How long does it take to see results from improved denial management?
The first wins come fast. The 48-hour rework rule alone typically recovers $5,000 to $15,000 in the first 60 days, because most practices have claims still inside the timely-filing window that nobody has touched. Structural improvements (cutting your denial rate from 12% to 5%) take three to six months.
Categories
Tag Cloud